Surveillance of mpox in the European Union/European Economic Area (EU/EEA) − Monthly report
Overview
This report presents data on mpox cases reported to the European Surveillance System (EpiPulse Cases). EU/EEA countries report case-based data to ECDC on diagnosed mpox cases. For case numbers by country, the Western Balkans and Türkiye are included.
The epicurve shown includes all mpox cases reported since 2022. The rest of the report includes data on the total number of cases in the past full 12 calendar months (July 2025 to June 2026).
Cases are analysed by date of diagnosis. This report includes cases reported to ECDC as of 17 July 2026.
Epidemiological summary
In June 2026, 129 mpox cases caused by clade I MPXV were reported by nine countries, with the largest number of cases being reported by Portugal (57). In May, 125 cases were reported by 13 countries, and in April, 167 cases were reported by 13 countries.
In June 2026, 22 mpox cases caused by clade II MPXV were reported by six countries, with the largest number of cases being reported by Germany (10). In May, 36 cases were reported by six countries, and in April, 47 cases were reported by seven countries.
In the past 12 months, 18 countries reported 829 clade I mpox cases and 18 countries reported 921 clade II mpox cases.
It total, 90% of the clade I mpox cases and 91% of the clade II mpox cases with complete information were reported among men who have sex with men.
Overall, 14% of the clade I mpox cases and 8% of the clade II mpox cases with complete information were hospitalised.
A total of 22% of the clade I mpox cases and 21% of the clade II mpox cases with complete information were vaccinated with two doses.
Epicurves
Total number of mpox cases – all clades – from Jan 2022 and as of July 17, EU/EEA
Total number of mpox cases by clade, by month of diagnosis in the past 12 months (July 2025 to June 2026), EU/EEA
Mpox cases by clade and country in the past 12 months (July 2025 to June 2026), EU/EEA
The five countries with the largest number of cases in the past 12 months are shown separately and all other countries that reported cases are grouped as ‘Other’
Maps
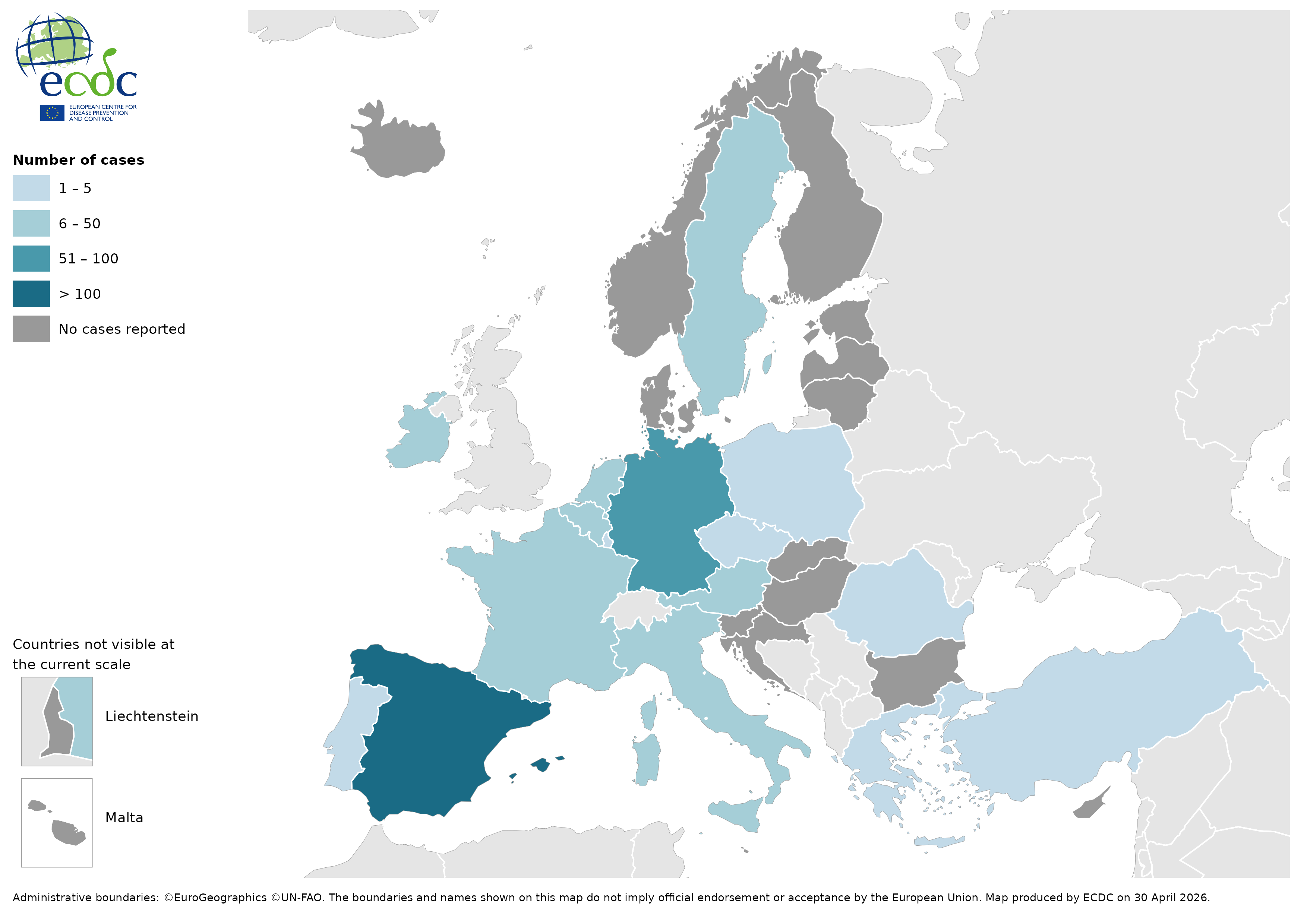
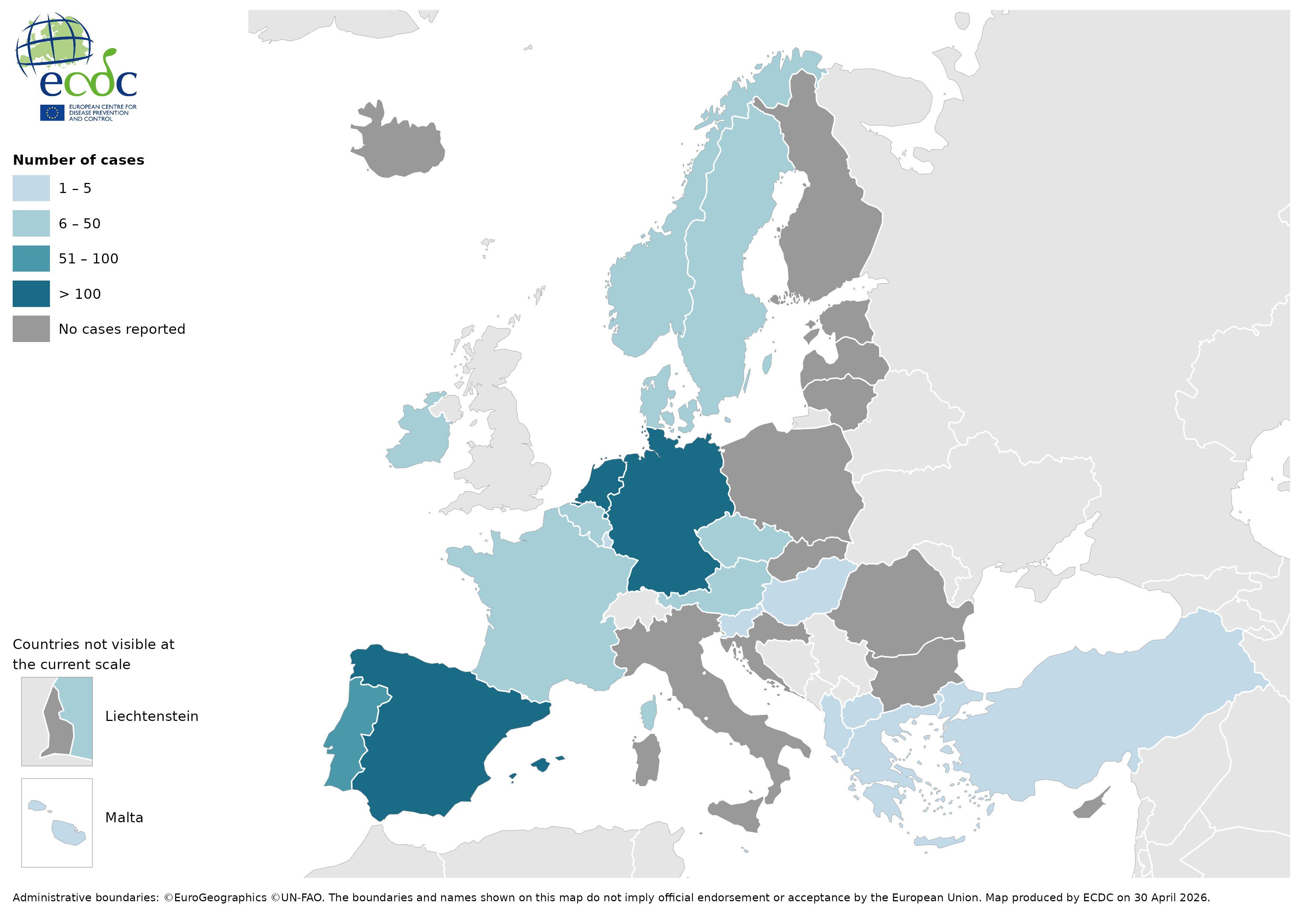
Mpox cases by clade in the past 12 months (July 2025 to June 2026), EU/EEA and the Western Balkans and Türkiye
Clade I
Clade II
TABLES
Mpox cases by clade in the past 12 months (July 2025 to June 2026), and past calendar month (June 2026), EU/EEA and the Western Balkans and Türkiye
Mpox cases by age and sex in the past 12 months (July 2025 to June 2026), EU/EEA

The distributions by age and gender of clade I and clade II are similar.
Mpox cases by sexual behaviour reported in people aged 15 years and above in the past 12 months (July 2025 to June 2026), EU/EEA*
The vast majority of mpox cases in clade I and clade II are among men who have sex with men.
Mpox cases by hospitalisation status in the past 12 months (July 2025 to June 2026), EU/EEA
The percentage of cases hospitalised is higher in clade I mpox cases than in clade II mpox cases.
In the past 12 months there have been two deaths reported in people infected with clade II. No deaths have been reported in people infected with clade I.
Mpox cases by vaccination status in the past 12 months (July 2025 to June 2026), EU/EEA
Among cases with known vaccination status, the majority of both clade I and clade II mpox cases are not vaccinated.
Mpox cases by travel status in the past 12 months (July 2025 to June 2026) and past calendar month (June 2026), EU/EEA
The proportion of travel-related cases has been low and similar between clade I and clade II over the past 12 months.
ASSESSMENT
The number of clade I mpox cases reported in the EU/EEA remains
relatively stable, while reported clade II mpox cases continue to
decline.
However, interpretation of short-term trends remains
limited because clade information is missing for a substantial
proportion of reported cases, and case and epidemiological information
may be updated retrospectively.
Clade I mpox case notifications
from the EU/EEA suggest ongoing transmission across the region,
primarily among men who have sex with men. In terms of severity,
hospitalisation rates remain low overall but are higher in clade I than
in clade II mpox cases. Information from Member States suggests that
clinical presentation is generally mild, including among hospitalised
cases.
ACTIONS
Increasing vaccination uptake is the single most important measure for mitigating the spread of both clades. Primary preventive vaccination (PPV) and post-exposure preventive vaccination (PEPV) strategies may be combined to focus on individuals at substantially higher risk of exposure and close contacts of cases, respectively, particularly in the event of limited vaccine supply. PPV strategies should prioritise gay, bisexual, and transgender people, and men who have sex with men, who are at higher risk of exposure. Strategies should also prioritise individuals at risk of occupational exposure, based on epidemiological or behavioural criteria. Health promotion interventions and community engagement are also critical to ensure effective outreach and high vaccine acceptance and uptake among those most at risk of exposure.
Further response options for EU/EEA countries include raising awareness among healthcare professionals, supporting sexual health services in case detection, contact tracing, case management, and making testing easily accessible.
ECDC’s ‘Threat Assessment Brief on the detection of autochthonous transmission of monkeypox virus (MPXV) clade Ib in the EU/EEA’ was published on 24 October 2025. It summarises information on the new cases, actions that EU/EEA countries can take, and the knowledge gaps that remain.
ECDC is continuously monitoring mpox in the EU/EEA and globally through event- and indicator-based surveillance, and remains in contact with partners. ECDC is in contact with affected countries to gather further information and consider response options.
Countries should continue efforts to sequence all positive cases and ensure that sequences are deposited in public repositories (European Nucleotide Archive (ENA), Sequence Read Archive (SRA), and/or GISAID EpiPox) or shared with ECDC through the EpiPulse platform or other means.